
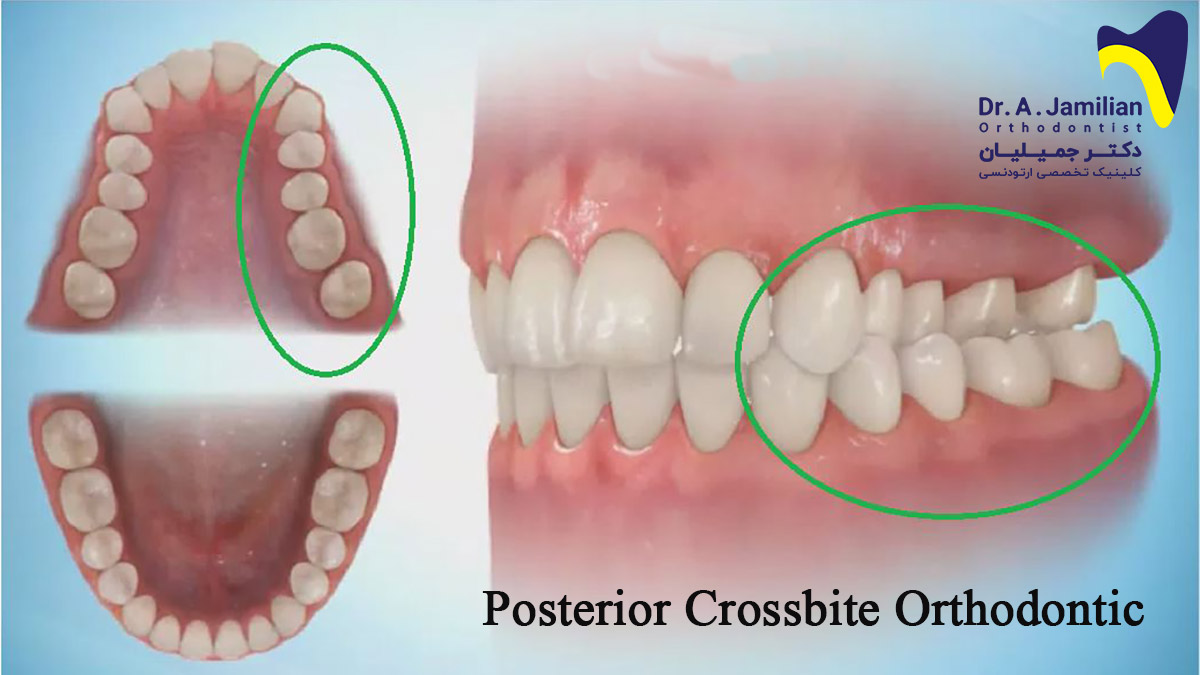
A patient visiting an orthodontist may be diagnosed with a posterior crossbite. This condition occurs during the mixed dentition stage due to the narrowed maxillary caused by a long habit of sucking. Children with a posterior crossbite are recommended to visit an orthodontist during their growth period to treat this malocclusion properly in the shortest time. When a posterior crossbite is decided to be treated through fixed orthodontics in an adolescent, orthodontists are recommended to begin the treatment with fixed or removable maxillary expansion appliances and continue with overcorrection and three months of retention.
Most full-cusp posterior crossbites are of the skeletal origin, whereas a unilateral posterior crossbite is often caused by teeth displacement. A posterior crossbite can cause maxillomandibular asymmetry. Clients are recommended to begin the treatment for posterior crossbites as soon as they are diagnosed with periodic dental checkups.
This treatment prevents not only dental abrasion but also mandibular shifts. This treatment is also irreversible unless skeletal problems cause the posterior crossbite. The orthodontist chooses the best treatment to treat a posterior crossbite taking into account its cause (dental or skeletal). Posterior crossbites with a dental origin can be treated by pushing and displacing teeth gently but continuously.

Main treatments for posterior crossbites in children
There are three primary methods for the treatment of moderate posterior crossbites in children.
Elimination of mandibular shifts by coordinating the upper and lower arches
Mandibular shifts may occur due to milk canines’ interference during the milk dentition stage or the late mixed dentition stage. In such cases, the posterior crossbite can be completely treated only by trimming and shortening the canines.
Maxillary expansion
The moderate bilateral maxillary stenosis can cause malocclusions, mandibular shifts, and posterior crossbites. As soon as such cases are observed, maxillary expansion should be performed to prevent oral or maxillofacial injuries. Severe cases of maxillary stenosis mainly do not cause a mandibular shift. Instead, maxillary teeth are located on the mandible. Considering the insufficient space in the maxilla in such patients, maxillary expansion providers more space and better conditions for the eruption of permanent teeth. Once diagnosed, a crossbite caused by narrowed maxilla should be treated both in the presence or absence of a mandibular shift.
Correction of dental arch asymmetry through dental displacement

In such cases, the following two methods can be used to correct posterior crossbites in children.
• Removable appliances with mini-screws: This technique’s success depends on the patient’s cooperation because such appliances can easily move inside the mouth.
• Adjustable lingual arches: The use of this appliance is considered the treatment of choice in preadolescent children. There are two types of adjustable lingual arches for this purpose.
A: W-arch. This is made of 36-mm steel wires allowing selective expansion of the maxilla either backward or forwards while applying the correct force if it opens 4-5 mm. A w-arch is placed 1-1.5 mm away from the soft palate and the edge of gums and extends up to 1-2 mm in the molar’s distal region.
B: Quad-helix.
This device has the following specifications:
- A quad-helix made of 38-mm steel wires is a more flexible appliance than w-arch.
- This appliance includes a helix and thus provides greater amplitude than w-arch. However, both appliances apply the same amount of force.
- The activation of anterior and posterior helixes causes the posterior and anterior expansion of the maxilla, respectively.
- A quad-helix is an appliance of choice for children with a crossbite, and the habit of finger sucking as the bulk helix in the anterior part of the palate can serve as a reminder.
- A quad-helix is the same as a w-arch in terms of the distance from the soft palate and the distal molar band’s extension.
The following points apply to both w-arch and quad-helix:
- Even if it is intended to treat dental extension, the midpalatal suture may slightly split in young children.
- The extension rate of the arch is 2 mm per month.
- The overcorrection is usually recommended to be done so that the palatal cusp of the upper molar comes into contact with the lingual slope of the buccal cusp of the lower molar.
- The active treatment usually takes 2-3 months, followed by a 3-month stage of retention.
- The orthodontist is recommended to remove the appliance out of the mouth and then cement it to the teeth (intraoral adjustment may cause unpredictable effects).






