Introduction
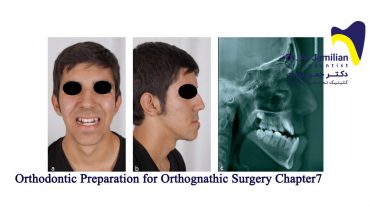
Skeletal class III malocclusion is characterized by mandibular prognathism, maxillary deficiency or some combination of these two features. The prevalence of Class III malocclusion varies among different ethnic groups, depending on the method of studying and age group of the patients. The prevalence in Caucasians ranges between 1% and 4%. A high prevalence has been reported in Asian population. Various studies have reported that 4% to 12% of Chinese and 9% to 19% of Koreans suffer from Class III malocclusion which is relatively higher than 0.6% to 1.2% reported for African Americans and 6% reported for Swedish people.
Approximately half of all skeletal class III malocclusions are reported to result from maxillary deficiency. More precisely, the incidence of Class III malocclusions suffering from maxillary deficiency was reported to be 65% to 67%. If the mandible of patients is markedly affected then the most common treatment would be orthodontic treatment in combination with orthognathic surgery. In this chapter, the main focus of attention will be on maxillary deficiency in growing patients.
In view of the high frequency of maxillary deficiency, maxillary advancement by orthopedic forces, is considered to be a viable treatment option in growing patients. A number of techniques have been described, including the use of a facemask, reverse chin cup, direct force application through implants placed in the zygomatic processes. It was also suggested that intentionally ankylosed teeth may be used as abutments for extra-oral traction in patients with a severe disturbance in maxillary growth. Miniscrew implants and miniplates have also been used to provide the necessary orthodontic anchorage in these cases. The tongue plate and tongue appliance have also been used for the correction of maxillary deficiency in growing patients. The mechanism of action associated with these appliances relies upon forward pressure from the tongue, which is transmitted via the appliance to the maxillary dentition and maxilla.
Treatment of maxillary deficiency in growing patients:
Growing patients with skeletal Class III malocclusion characterized by maxillary deficiency can be treated by either extra oral or intra oral appliances. extra oral appliances include facemask, reverse chin cup, reverse headgear, and protraction head gear and intra oral appliances include tongue appliance, fixed tongue appliance, tongue Plate, Frankel III, miniplate in combination with Class III elastics, miniscrew in combination with Class III elastics.
Extra-oral Appliances
1.1 Facemask
Face mask therapy has become a common technique used to correct the developing Class III malocclusion. A search in literature will reveal copious researches about face masks and their effects on nasomaxillary complex. In addition, the experimental studies constantly demonstrate pronounced forward movement of the maxilla due to heavy and continuous protraction forces of face masks.
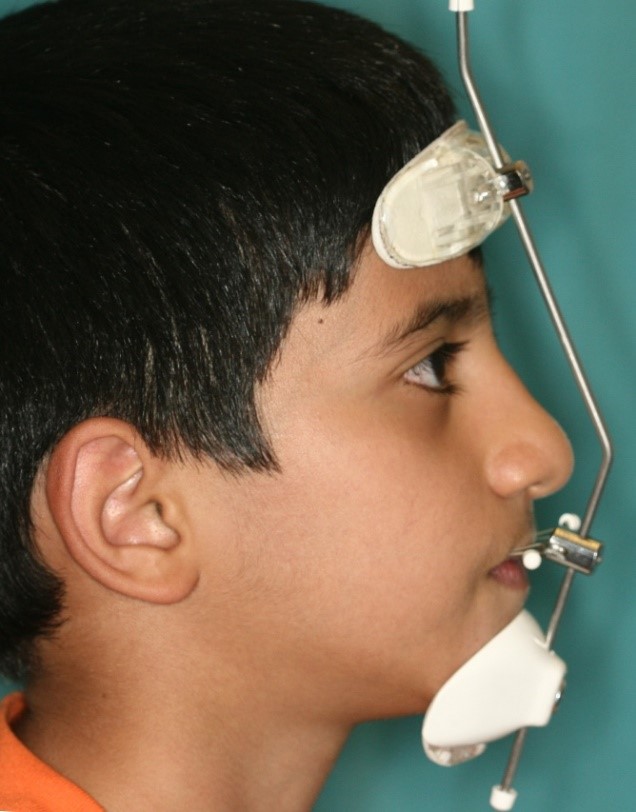
Face masks were first described more than a century ago. Delaire et al’s facemask promotes midface orthopedic expansion with slight inferior and anterior movement of the maxilla. The protraction face mask provides a direct constant anterior force to the maxilla with downward and backward rotation of the mandible. Nanda introduced a modified protraction headgear that aimed to control the point and direction of force application. (Figure 01)
Similar appliances to facemask have been proposed by various clinicians which vary slightly from each other but their mechanisms are almost the same. Some of these appliances are reverse headgear, front pull headgear, protraction headgear and so on.
Limitations
However, one of the problems with face masks is their bulky size and shape, which make it a discouraging choice for children. Especially patients who wear glasses will be more susceptible to discomfort. This discomfort along with the embarrassment caused by the large size for children, especially at school in front of other peers, might reduce patient compliance. In facemask, the forehead and the chin are used as areas of support. Nanda reported that in facemask therapy although maxilla would translate forward; downward and backward rotations of mandible are unavoidable. The backward and downward rotation of the mandible is unfavorable in vertical growth pattern patients. On the contrary, this effect would be favorable in patients with horizontal growth pattern. Facemask would also cause forward movement of the maxillary dentition and lingual movement of the mandibular incisors.
1.2 Reverse chin cup
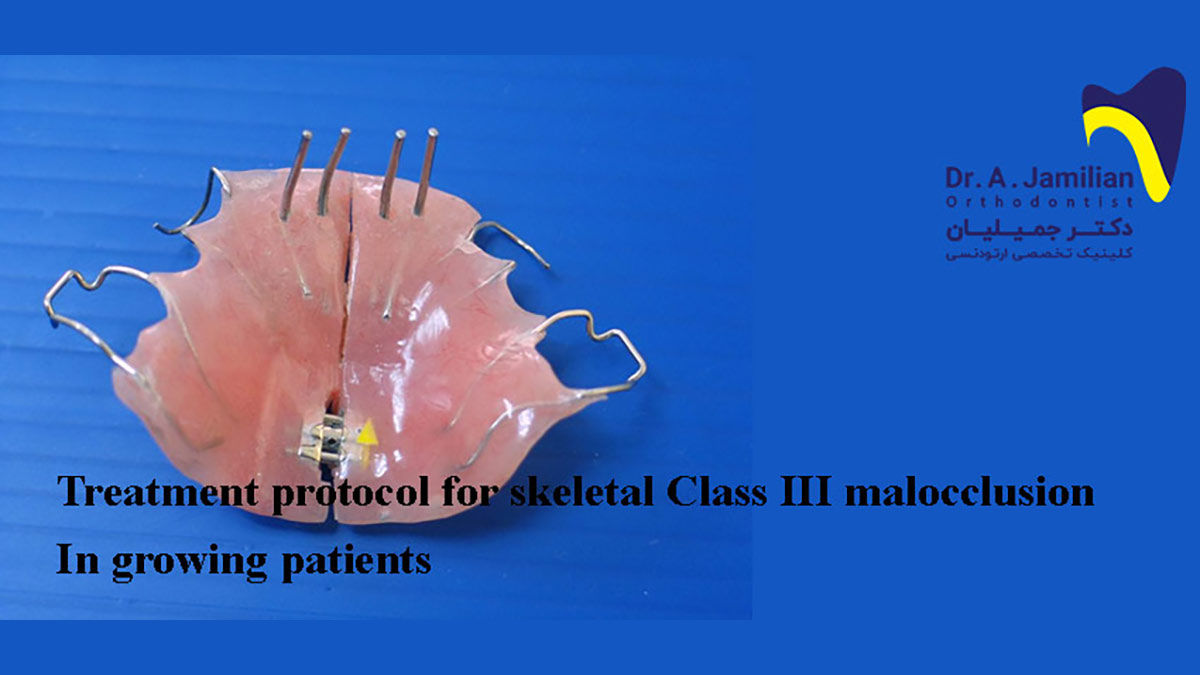
Reverse chic cup is an extra oral appliance first introduced by Showkatbaksh et al.8,22 Reverse chin cup is composed of an upper removable appliance and a custom made porous acrylic chin cup with two vertical arms. The upper removable appliance consist two Adams clasps on the permanent first molars, two C clasps on the primary canines and two C clasps on the permanent central incisors. If necessary, the number of C clasps and Adams clasps can be increased for anchorage reinforcement. The end of each arm of the chin cup is bent to form a hook. Two orthodontic latex elastics (recommended: 5/16, heavy) connect the hooks of the palatal canine area of the upper removable appliance to the hooks of reverse chin cup in order to deliver approximately 500 g of force on each side. A high pull head cup is used to hold the reverse chin cup. The patients are instructed to wear the appliance full-time except for eating, contact sports and tooth brushing. (Figure 2)
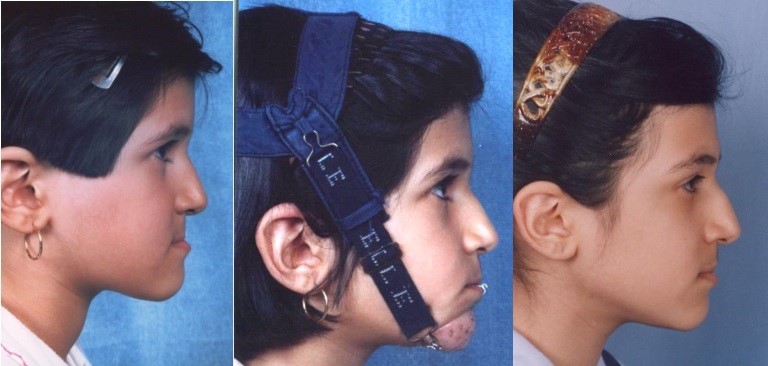
Concave profile was obvious in her. She had a reverse overjet, and underbite. She was treated by reverse chin cup. After 18 months of treatment her profile was improved and a positive overjet was achieved.
Reverse chin cup is very similar to facemask and is able to produce forward movement of the maxilla in growing patients; however, chin cup may be more favorable for patients due to its smaller size.
download link of, Treatment protocol for skeletal Class III malocclusion in growing patients