Abnormal breathing through the mouth instead of the nose imposes pressure on the jaws and gradually results in maxillary stenosis due to the nose’s negative pressure. Thumb sucking can also lead to maxillary stenosis due to pressure imposed on cheeks. In addition to this bad habit, other factors can result in mouth breathing.
- Chronic allergies that continuously close the nasal airways
- Nasal polyps
- Large tonsils
Maxillary Stenosis Complications
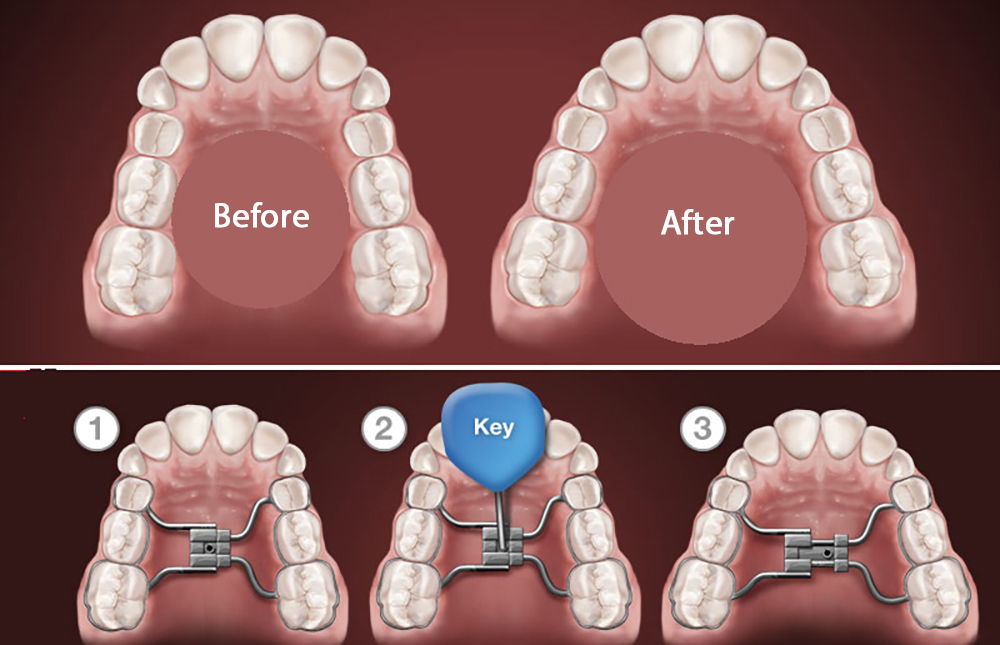
The first complication of this condition is crowded teeth. The following picture depicts the teeth before treatment of the maxillary stenosis. As shown, the upper teeth do not cover the lower teeth, especially in the posterior teeth and the anterior ones. This disorder occurs due to a small and dome-shaped maxilla. Dome-shaped maxilla refers to a deep palate and deep jaw, which can be felt when the tongue touches the palate. This anomaly gives the patient an ugly appearance when speaking. Moreover, improper and non-standard contact of the teeth results in incomplete chewing and grinding of the food, leading to digestive disorders. The tongue also gets stuck in these gaps and exacerbates the condition.
A maxillary stenosis can also affect speaking and disrupt the expression of words that require the tongue’s contact with the palate or upper teeth. A maxillary stenosis can also cause narrowing of the nasal cavities, nose malformation, and nasal airways disruption.
When does a maxillary stenosis initiate?
The disorder may initiate from infancy when the baby begins sucking his/her thumb. Respiratory diseases and allergies are developed and become chronic after 8-9 years, resulting in a small upper jaw in the long term.
Maxillary stenosis treatment methods
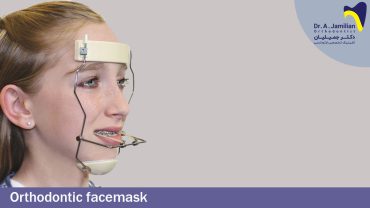
First, the maxillary stenosis’s cause, for example, the thumb sucking or abnormal breathing, should be resolved. Meanwhile, the orthodontist puts an intraoral device in the palatal area and maxilla to impose pressure on the maxilla’s side bones. As seen in the figure below, the teeth are inclined toward the outside, modified through orthodontics.
It is suggested to visit an otolaryngologist during the orthodontic treatment to take the necessary measures if the problem is due to abnormal breathing.

Sometimes the problem has a genetic and congenital background. In this case, the treatment should be initiated once primary or permanent teeth are erupting, i.e., at the age of 6-7. When the maxilla is forcedly opened, the teeth will align in a bigger arch, providing greater teeth alignment space.
It is suggested to perform the orthodontic treatment and otolaryngologist visits simultaneously; otherwise, the teeth will return to their previous position as the wires are removed because the problem’s primary cause, i.e., abnormal breathing, is not resolved. The disorder will be recurred after removing the orthodontic wires.
Some patients have an oversized tongue or positioned in the front of the mouth, leading to the tongue’s magnified appearance. When the tongue is large to reach the chin or the nose, the patient should visit an otolaryngologist. Surgery is performed on the tongue to reduce its size by removing its middle part to avoid damage to the gustatory sense, usually after orthodontics.