Open Bite
This case report demonstrates a 22.4 year old girl with skeletal Class I malocclusion.
Summary:
The patient had aggravated arch length deficiency due to concurrent crowding and dentoalveolar protrusion. She also had severe open bite. Molars and canines were in Class I relationship on both sides. She was a vertical growth pattern patient and the lips were closed with strain.
Examination of head and face:
On the frontal plane the patient presents a symmetric face with good facial proportions. The profile analysis reveals a slightly convex profile and lip incompetency.
Functional examination:
Patient showed no lateral or sagittal shift of the mandible when closing. Her TMJs were asymptomatic and no history of TMD or headaches was reported by the patient or parents. Maximum jaw opening was within normal range. No muscle pain could be detected on palpation. Centric occlusion and centric relation were coincident.
Intra-oral examination:
The patient was in her permanent dentition with all teeth present except for the third molars. Dentoalveolar protrusion and crowding in both jaws were obvious, which were indicative of the patient’s arch length deficiency. The patient also had severe open bite.
She had fair oral hygiene with good overall periodontal status. One restoration could be seen on 26.
Treatment plan:
The patient’s chief complaints were:
- Open bite
- Bimaxillary protrusion
- Crowding in upper and lower jaws
The age of the patient made here treatment difficult and it had to be considered that the patient had aggravated arch length deficiency due to both severe crowding and bimaxillary protrusion. Excessive protrusion of incisors, open bite and crowding are usually an indication for premolar extraction and retraction of the protruding incisors. Therefore, the treatment option decided for the patient was extraction of the first premolars in both arches (14, 24, 34, & 44). These extractions would create more space for canine retraction. Nevertheless, maximum anchorage had to be done to prevent the mesial movement of the posterior teeth. The purpose of the extractions was to use all the space created by retraction of the canines for relieving the crowding and correcting the bimaxillary protrusion and open bite. Ideal overjet, overbite and competent lips would also be achieved followed by these treatments.
Treatment results:




The patient’s appearance improved substantially after the treatment and her bimaxillary protrusion was corrected to a satisfactory degree. Upper and lower incisor inclinations were corrected which led to retraction of upper and lower lips. The patient’s open bite was successfully corrected and normal overbite and overjet were achieved. No sign of crowding could be seen in the upper and lower jaws. Her TMJ remained asymptomatic with no clinical signs or symptoms. The patient has a pleasing profile with competent lips. Upper posterior bite plate was used because the patient was a vertical grower and lower Hawley retainer was used in order to get better stability. She was referred to a general dentist in order to extract her third molars. The retainers were worn on a full time basis for the first 6 months then on a part time basis after which their use was discontinued.
Retention:
One year and two months after retention and two years and two months after the end of treatment the profile is still satisfactory and the lips are competent. No sign of dentoalveolar protrusion can be seen. The patient has a pleasant smile. The intercuspation improved and molars and premolars are in a more stable Class 1 occlusion with satisfactory overjet and overbite. No sign of crowding, open bite, and upper and lower incisors’ flaring can be seen. No signs or symptoms of TMD could be detected in the patient.
Cephalometric Data:
| Pretreatment | Posttreatment | Mean SD | ||
| Sagittal Skeletal Relations | ||||
| Maxillary Position S-N-A | 81° | 81 º | 82º± 3.5º | |
| Mandibular Position S-N-Pg | 77° | 77 º | 80º ± 3.5º | |
| Sagittal Jaw Relation A-N-Pg | 4° | 4 º | 2º ± 2.5º | |
| Vertical Skeletal Relations | ||||
| Maxillary Inclination S-N / ANS-PNS | 13° | 11 º | 8º± 3.0º | |
| Mandibular Inclination S-N / Go-Gn | 42° | 42 º | 33º± 2.5º | |
| Vertical Jaw Relation ANS-PNS / Go-Gn | 27° | 29 º | 25º± 6.0º | |
| Dento-Basal Relations | ||||
| Maxillary Incisor Inclination 1 – ANS-PNS | 116° | 106 º | 110º± 6.0º | |
| Mandibular Incisor Inclination 1 – Go-Gn | 108° | 92 º | 94º± 7.0º | |
| Mandibular Incisor Compensation 1 – A-Pg (mm) | 6 mm | 2 mm | 2 ± 2.0 | |
| Dental Relations | ||||
| Overjet (mm) | 3 mm | 2 mm | 3.5 ± 2.5 | |
| Overbite (mm) | -4 mm | 2 mm | 2 ± 2.5 | |
| Interincisal Angle | 110° | 129 º | 132º ± 6.0º |
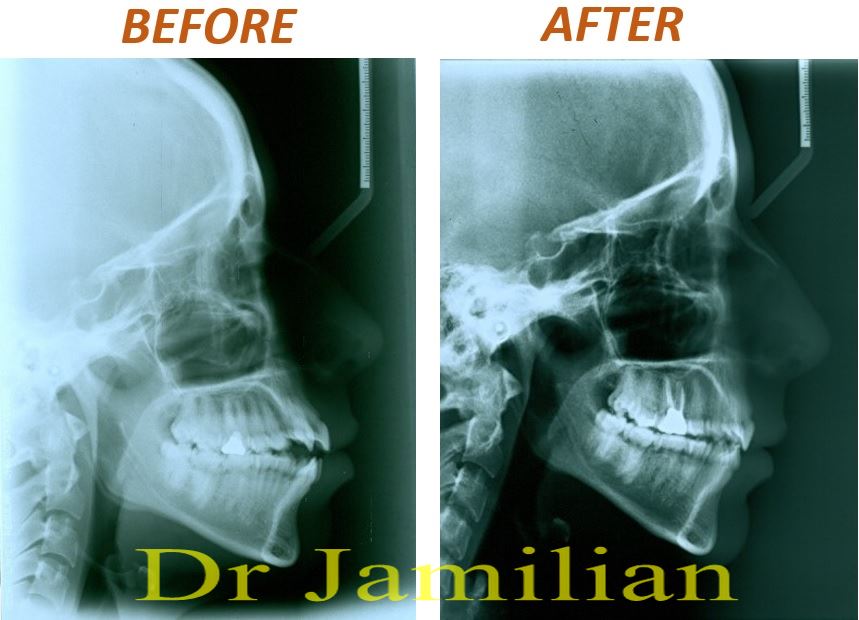
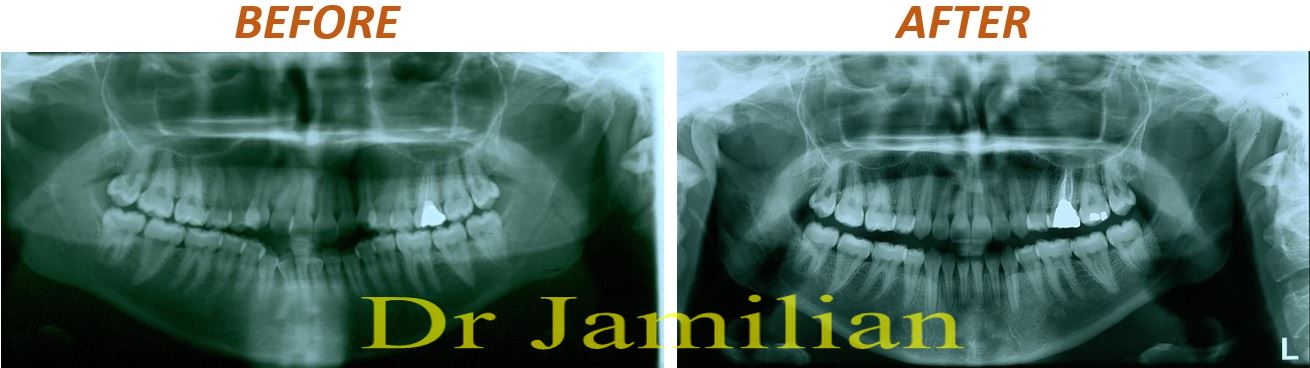
The following images show the pre and post treatment lateral cephalogram and OPG of the patient: